

Link to full post: Why don’t we screen healthy people to catch diseases early? | Out-Of-Pocket
The fight that comes up every month:
"Let's do more scans"
But it's not exactly a cost thing. Doing more tests can actually cause more harm than they help.
What happens when we screen lots of healthy people?
First, let's refresh ourselves on sensitivity and specificity. These tell us how good a test that's trying to find a disease is.
Sensitivity - the probability that if you have a disease, the test will detect it.
Specificity - the probability that if you DON'T have the disease, the test will say you don't have the disease.
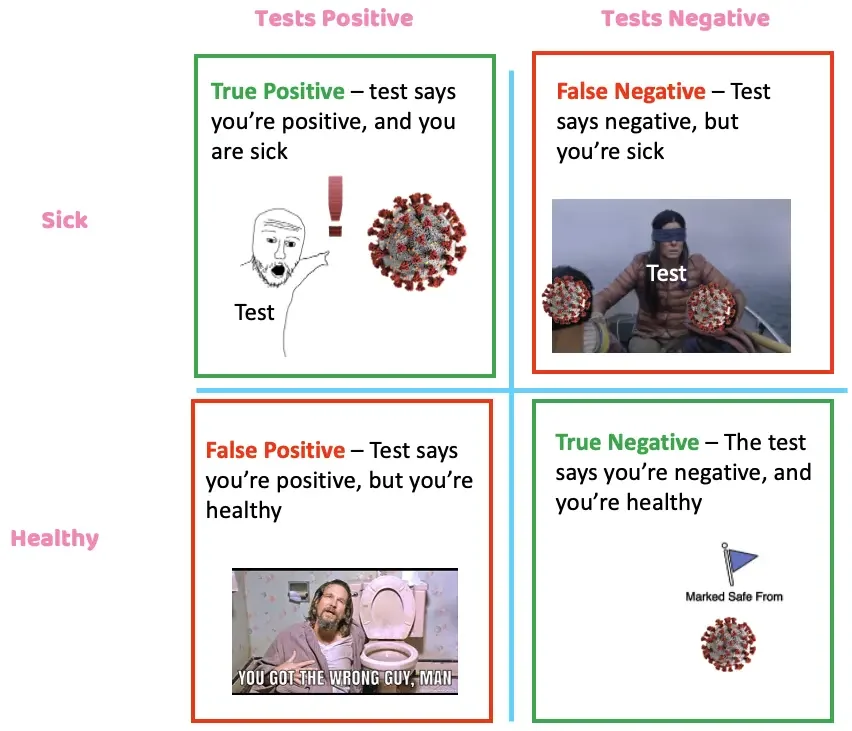
Ideal tests are great at both. Unfortunately, the reality is that most tests make a trade-off between the two.
Let's give an extreme, theoretical example. The prevalence of Nikhilitis in the population is 1:1,000. It causes incontinence, erectile dysfunction, generally bad vibes, and a 1% chance of death.
We've developed a test with a sensitivity of 99% and a specificity of 90% in detecting Nikhilitis. A real estate investor on Twitter goes viral about how everyone NEEDS to get this test. So about 1,000,000 healthy people show up to get screened.
Out of the 1M, we know that 1,000 of those people have the disease.
If we test all 1M, the test will correctly catch 990 of them and miss 10 of them thanks to the sensitivity.
However, where it really gets dicey is false positives. Remember, 999K people came in that DO NOT have Nikhilitis and the test has a 90% specificity, which yields 10% false positives.
Thanks to a 90% specificity, 99,900 people in that group will get a false positive test. So we correctly identified 990 people that had Nikhilitis, at the expense of 99,900 false positives.
Now we need to follow up with everyone that got a positive test result and do a biopsy. Let's say a confirmatory diagnosis for Nikhilitis is a lobotomy with a .1% mortality rate. If Nikhilitis only causes 1% chance of death, was this worthwhile to do on everyone?
- 99,900 false positives + 990 correctly positive = 100,890 that need biopsies
- 100,890 need biopsies * 0.1% mortality rate = 100.89 deaths from biopsy
Vs.
- 990 correctly positive * 1% chance of death from Nikhilitis = 9.9 people saved
So in the end, we killed 101 people to save 10 people. This is an extreme example to illustrate the point, but you can see how large these false positive numbers get (even with a pretty good test!) if you just haphazardly screen the entire population. That's why there are guidelines in place for who should be screened - you want to limit it to a population that has a higher likelihood of having the disease.
The Four Main Problems when Healthy People are Screened
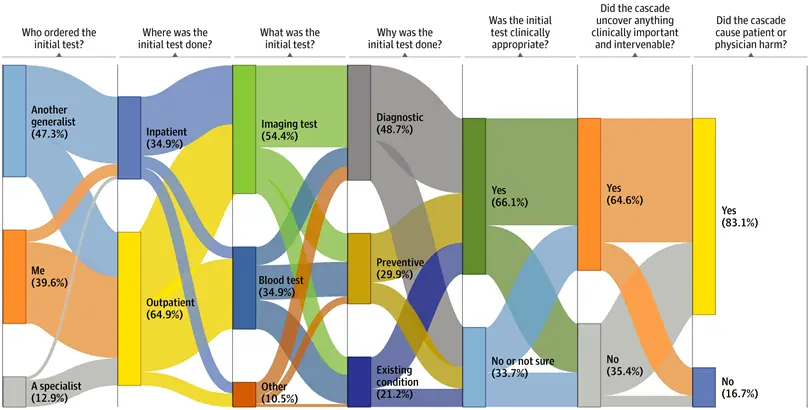
Lots of follow up tests - If something irregular is found during a screen, a whole host of downstream things will need to happen to confirm or throw out a possible diagnosis. These are called treatment cascades. There's a good paper that shows how these cascades can catch things clinically important (64.6%), but in a vast majority of cases, they cause some harm financially, psychologically, or physiologically (83.1%).
Physical harm during biopsies - Many biopsies are invasive and can really harm you or mess up your quality of life. About 10% of lung cancer biopsies caused a pneumothorax. Liver biopsies cause a fatal hemorrhage in 4/10,000 cases. Those small percentages start adding up if everyone were to suddenly get these tests.
You would've been fine anyway - If you look hard enough and long enough, you'll find something wrong with everyone. Even if you have a disease, you might be fine without treating it anyway. For example, you might have cancer, but it could be slow growing and not causing any symptoms to the point where it didn't even take any years off your life.
Wasting time, money, and resources - Reducing the number of "low value tests" that create a lot of unnecessary downstream work and cost seems like a great place to target.
Cancer screening Gone Wrong - Prostate and Thyroid
In the late 1980s, the prostate-specific antigen (PSA) test was approved by the FDA. However, starting in 2008, a few large studies started coming out with different information. Some studies suggested the screening test was actively harming people due to biopsy and treatment complications.
Part of the reason was the fact that prostate cancer is largely a very slow growing cancer, and most people actually end up dying with it instead of from it. The PSA test couldn't really tell if it was a slow or fast cancer.
From 1986 through 2005, one million men received surgery, radiation therapy or both who would not have been treated without a PSA test. Among them, at least 5,000 died soon after surgery and 10,000 to 70,000 suffered serious complications. As a result, Richard J. Ablin, who in 1970 discovered a prostate-specific antigen, has called its widespread use a 'public health disaster'.
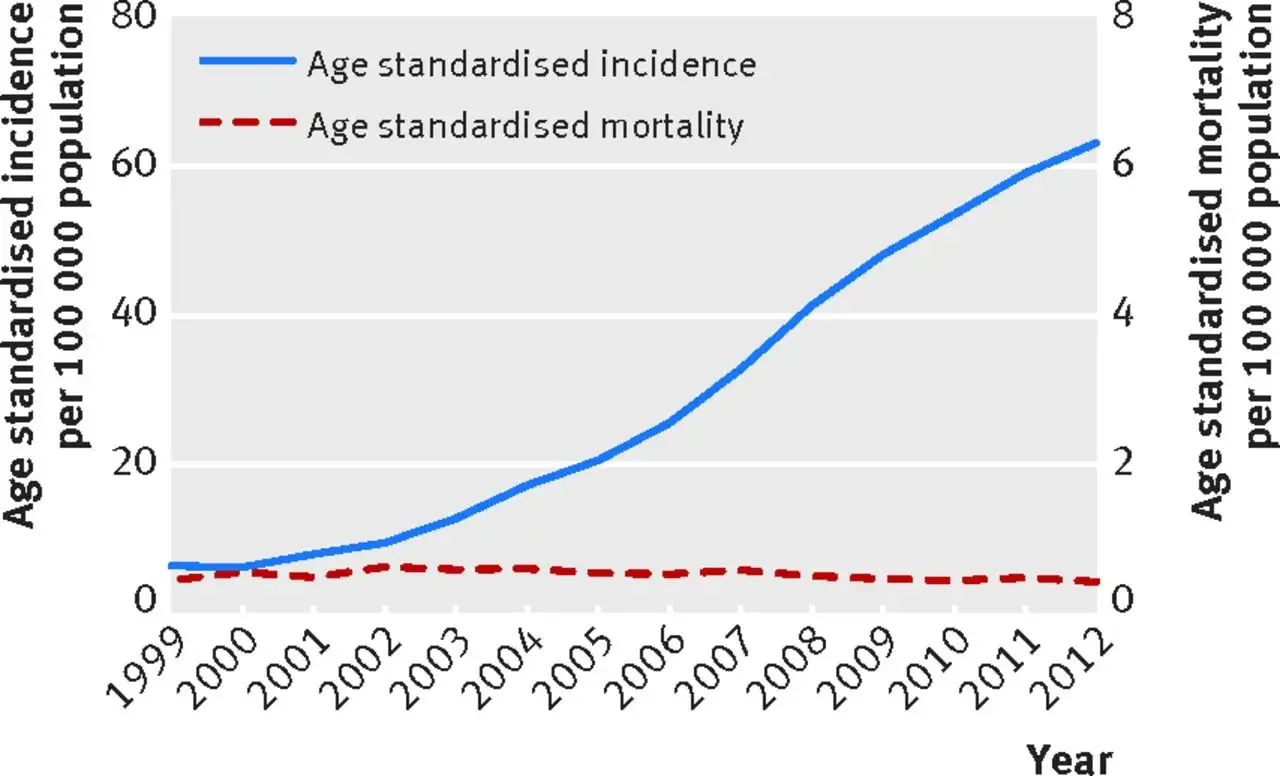
In Korea, they started doing widespread screening for cancer in 1999. Thyroid cancer incidence skyrocketed, but mortality rates due to thyroid cancer basically were unchanged, which suggested that increasing the screening wasn't changing anything. Instead, people were subject to a battery of tests and treatment for no reason.
Current Issues with Rolling Out Screening
The value of a life - The uncomfortable truth that no one wants to say explicitly when designing these screening guidelines is, "We're comfortable with missing ____ cases of a disease that might cause ____% death. This is to prevent _____ people from getting unnecessary tests/procedures, which in itself would cause ______ deaths and other costs."
The difficulty in evaluating if a screen is working - It can take decades to know if a screen actually reduces mortality, and by then, good luck changing anyone's mind.
Trust - Patients trust doctors who "do something," and ordering tests feels like doing something. This is compounded by all the incentives doctors have to order tests anyway—fee for service, malpractice avoidance, patient satisfaction scores.
What level of risk do we want patients to choose? - If patients understand the risks of over-testing and want to pay out-of-pocket anyway, should we let them? Some find it paternalistic to say no; others point out only the rich can pay; others argue patients will always think "it won't happen to me." That tension sits at the core of US healthcare.
The impact of lawsuit culture — "No one ever sends you a thank you note for not ordering a CT scan." - Dr. Eric Funk
What level of risk do we want patients to choose? — If patients understand the risks and want to pay out-of-pocket, should we let them? That question sits at the core of US healthcare.
The Future of Screening
Changing evidence-based guidelines for screening - I think one issue is that the screening guidelines aren't yet personalized enough. As we get more personalized data + cohorting of patients like us, we'll understand which subpopulations have higher prevalence of disease. That should yield more personalized screening guidelines.
Blood based biopsies - The new wave of liquid biopsies that scan for signs of cancer is going to be the real tipping point for this discussion. Grail's Galleri test isn't FDA approved but has a CLIA waiver, so people or employers can pay for it out-of-pocket.
Patients are going to see ads about a blood test that can find cancer and have a lot of questions about how to get it themselves. Payers are going to get a lot of shit for not covering them. This feels like when the dam breaks.
Will short term pain create long term solutions? Maybe screening the population will create a lot of false positives in the short term, but as a result, we could see increased demand for safer biopsy methods, clinical trials that start at earlier stages in the disease, personalized health baselines for more people that can be used for research down the road.
Conclusion
I actually think asymptomatic screening is an important conversation with non-obvious answers to reasonable questions. And I hate that whenever this comes up online, it gets so disrespectful and condescending. It really brings out the worst of doctors as gatekeepers and tech people as know-it-alls.

This conversation will also get even more important as diagnostics and screening tools become more specific and widespread.
Thinkboi out,
Nikhil
